Stockhouse recently presented our audience with an introduction to Nash Pharmaceuticals (a wholly-owned subsidiary of Breathtec Biomedical Inc (CSE: BTH, OTCQB: BTHCF, Forum), in the form of a three-part series. For your convenience, we have compiled that series into a single article.
NASH Pharmaceuticals 1: Fast-Tracking Pharma Success
 Drug repurposing? It doesn’t sound very sexy. In fact, it is the key to a pharmaceutical treasure chest.
Drug repurposing? It doesn’t sound very sexy. In fact, it is the key to a pharmaceutical treasure chest.
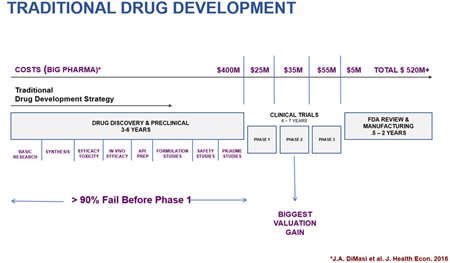
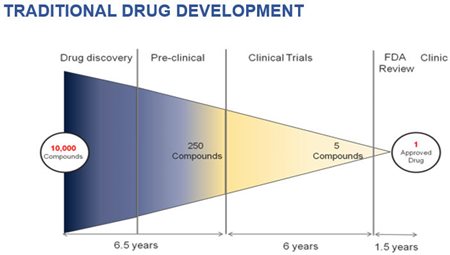
Today, developing new drugs has never been so expensive and time-consuming. From the initial “discovery” phase through to the completion of the formal clinical trials necessary for licensing, this process can eat up as much as 15 years, with costs in some cases exceeding half a billion dollars.
If that isn’t daunting enough for pharmaceutical companies, 90% of new drug candidates fail before ever reaching the stage of actual human testing. Yet because of the time/expense/risk inherent in this process, even a single drug success can mean a payoff in the $100’s of millions for a drug company and its shareholders. In some cases, the reward is in the billions.
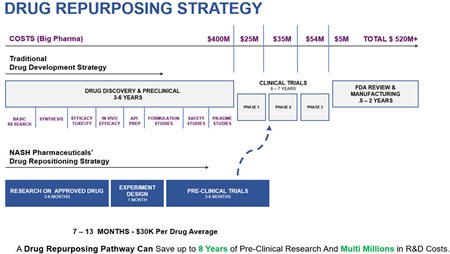
Drug repurposing, as its name implies, involves finding a new therapeutic application for an existing, approved drug. This approach can save as much as 8 years of R&D time and $10’s of millions in development costs. Suddenly, drug repurposing looks much sexier to investors.
Enter NASH Pharmaceuticals Inc. (CSE: BTH, OTCQB: BTHCD, Forum), a wholly owned subsidiary of Breathtec Biomedical Inc. A brief explanation is in order.
NASH Pharmaceuticals was a private biopharma company. Breathtec is a health technology company specializing in medical device development, that was looking to add a drug development division.
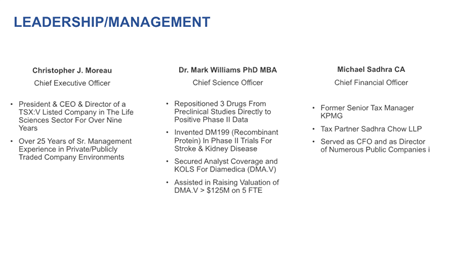
In the fall of 2017, NASH’s CEO Christopher Moreau was looking for new ideas for the Company’s drug research program. Opportunity knocked in the form of a renewed acquaintance.
Dr. Mark Williams (now NASH’s Chief Science Officer) was an experienced drug development scientist in the pharmaceutical industry. Among the projects in which he had taken a lead role was “repositioning” multiple drugs for new medical applications.
Williams was fascinated with the research and commercial potential of drug repurposing and began investing his personal time and energy over 5 years doing his own research in this area. Moreau and Williams had met 12 years earlier, having previously worked together for the same biotech company.
A chance encounter led to coffee. The two began to talk about their current work, and the NASH Pharmaceutical business model was born. Moreau introduced Williams (and his research) to the Nash Board of Directors and the Board was equally enthused with the commercial potential of this drug repurposing strategy. Dr. Williams became the Chief Science Officer for NASH.

To close the loop, Breathtec Biomedical recently “acquired” NASH Pharmaceuticals, but it is the NASH management team and unique business model that are now the focal point of operations.
Of great interest to investors is that when Dr. Williams was introduced to the NASH Board in early 2018, he brought more with him than just an exciting concept. He also brought thirteen previously approved drug candidates that were ready for fast-track screening, all potentially leading to the enormous payoffs previously outlined. More on this later.
Here investors not familiar with the pharmaceutical industry require a little educating. Drug development begins with pre-clinical research. This is the process starting from initial discovery that culminates in animal testing for the potential drug candidate.
Success at the pre-clinical level eventually leads to human “clinical trials”. This is formal testing of the potential drug on human patients and it is comprised of three phases. A Phase I clinical trial is devoted to establishing the safety and tolerance of the potential drug in human patients.
(click to enlarge)
This is where the drug repurposing strategy exhibits such strength as a business model. These drugs that are being “repurposed” have already been through the approval process once. This means that safety and tolerance (the objective of a Phase I trial) has already been established. Thus, drug repurposing is a drug development short-cut that allows the developer to leap-frog all of the many years of pre-clinical work and a Phase I clinical trial and move directly into a Phase II trial.
It is at the Phase II stage where the efficacy of a potential drug is tested (and hopefully demonstrated). It is this stage where the drug development process becomes of enormous interest to Big Pharma. The numbers here speak for themselves.

It is here where the pharmaceutical industry shifts gears from looking at the scientific potential of a drug candidate and becomes squarely focused on the commercial potential. Here Big Pharma has never been so interested in (and so dependent upon) the junior pharma companies doing the majority of such research.
The hunger of multinational pharmaceutical companies for new drugs (that can be patented) can be summed up in three words: the Patent Cliff.
The Patent Cliff is the label that the pharmaceutical industry has attached to the rapid depletion of patented drugs already developed by the major drug companies. Not only have these drug patents expired for a long list of licensed drugs, but many of the expired patents are for major revenue-producers for Big Pharma.
At the same time that is has never been more difficult and expensive to bring new patented drugs to market, drug-makers saw patents expire (in 2017 alone) on drugs with total annual revenues of $26.5 billion. But last year wasn’t even the worst year for Patent Cliff losses for Big Pharma.
In 2012, patents expired on licensed drugs with total annual revenues of $55 billion. And the moment that a drug loses patent protection, revenues for the patent-holder can fall by as much as 80%. Ouch.
With such huge holes to fill in their pipelines and drug development so intensely expensive and time-consuming, it is simply not feasible for these multinational drug companies to replenish their drug pipelines through internal R&D alone. Increasingly, Big Pharma is forced to buy new drugs to restock its own drug cabinet.
So if drug repurposing is such an efficient strategy for addressing a huge, known problem, why isn’t everyone doing it? Dr. Williams explains how and why this isn’t nearly as simple a process as it sounds.
“In order to even have a chance for a successful drug repurposing program you need to be able to file a new patent for the old drug, once your research confirms that it can treat a new disease. For this to occur, the idea, the concept, the scientific approach needs to be completely novel, one that has not been thought of before or even written about in order for you to be able to file a new patent…and there in lies the most challenging part.
How does one come up with a new idea about how a drug works in the body and could therefore possibly treat a new disease, that’s totally new? That’s the catch. For the Nash Pharma program, it was a combination of years of intense research with some good luck thrown in.”
Not as easy as it sounds. Even if a junior pharma company can find a promising drug to repurpose that isn’t unpatentable because of “prior art” or out-of-bounds because another drug company has already pioneered such research, researchers still have to find therapeutic applications for these repurposed drugs that actually work.
This is a process not unlike finding the proverbial needle in a haystack. This leads back to what Williams brought to the table when he joined NASH Pharmaceuticals: thirteen viable drug repurposing candidates that could be screened, repurposed, and then quickly advanced to a Phase II clinical trial. CEO Moreau estimates that these drugs can be readied for Phase II trials at a rough average of 7 – 13 months time, and at a cost of approximately $30,000 per drug.
(click to enlarge)
What are these thirteen “needles”? What is the commercial potential of NASH’s lead R&D programs? What are other companies worth that have brought such drugs to market?
In Parts II and III of Stockhouse’s first multi-part series, investors will learn the answers to these questions and more.
The world needs new drugs. The combination of aging populations and greater health expectations are increasingly making us drug-dependent populations. In the United States, more than 40% of all Americans over the age of 18 are on some form of prescription drug regimen.
Big Pharma needs help. NASH Pharmaceuticals sees its drug repurposing business model as not only the solution for this major health issue, but as the means to unlock pharmaceutical riches that could easily total in the billions of dollars – for this $12 million junior pharma company.
breathtecbiomedical.com
Nash Pharmaceuticals 2: Scaling the Patent Cliff
 The Patent Cliff. It’s real. It’s big. And it’s a really big headache for Big Pharma.
The Patent Cliff. It’s real. It’s big. And it’s a really big headache for Big Pharma.
Every year, drug patents expire on licensed pharmaceutical products with revenues in the billions of dollars. Losing patent protection can mean the instant loss of up to 80% of revenues for the patent holder.
However, going back now more than a decade, there has been a large wave of patent expirations covering drugs with total revenues in the $10’s of billions – each year. In 2012 alone, Big Pharma lost patent protection on licensed drugs with total revenues of $55 billion.
These are enormous holes to fill in the drug pipelines of Big Pharma, and this comes at a time when drug development has never been so time-consuming and never been so costly. Nash Pharmaceuticals, a wholly-owned subsidiary of Breathtec Biomedical Inc. (CSE: BTH, OTCQB: BTHCD, Forum), has created a business model that can open up new patent life on old drugs.
In Part 1 of this three-part series; Stockhouse readers learned how and why this junior pharma company sees itself as a significant cog in bringing drugs to a patent-ready stage (quickly and cost-effectively): drug repurposing. In an industry where even a single new patent can be worth $100’s of millions (or sometimes billions), this is a $12 million tech junior with home-run potential.
(click to enlarge)
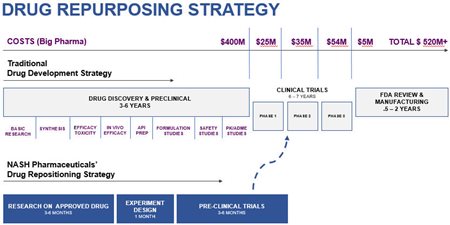
A repurposed drug has already completed all of its preclinical work (for the original disease it was used to treat). Thus this drug repurposing business model could allow Nash to shave up to 8 years off the total time to market timeline. It can also save millions (or even tens of millions) of dollars on drug development costs.
In Part 2, readers will get specifics about the current focus of Nash’s R&D. As noted in Part 1, via years of prior research from Chief Scientific Officer, Dr. Mark Williams, the Company has already screened thirteen potential candidates in order to identify compounds that could be quickly moved through into a Phase II (human) clinical trial.
What is the significance of reaching Phase II clinical trials? For readers who haven’t read Part 1, a Phase II clinical trial is the stage of research where drug companies formally demonstrate the efficacy of the (potential) new drug. For this reason, being able to cross this Phase II threshold is where these drug discoveries start to achieve their commercial potential.
(click to enlarge)
As noted in Part 1, fast-tracking repurposed drugs to the point of human trials is a multi-stage process: identify drugs for screening (difficult/time-consuming), test in animals, file new patents, advance (directly) to Phase II human trials.
Of the original 13 candidates, and through its ongoing research programs, Nash has developed data that supports the advancement of up to 7 drug candidates into Phase II studies. In previous releases, Nash has already announced that a number of the candidates outperform current standard of care therapies when they were tested in animal models.
That’s 7 opportunities to swing for the fences right now. In addition to researching new candidates for repurposing, some of the 7 top performing candidates can be screened for additional disease indications.
At the top of the Company’s list in advancing repurposed drugs to Phase II trials are three candidates, representing new treatments for:
- Non-Alcoholic Steatohepatitis
- Inflammatory Bowel Disease
- Chronic Kidney Disease
Investors lacking a medical background will most likely be more familiar with the latter two medical conditions. However, it is actually Non-Alcoholic Steatohepatitis (or “NASH” disease) that is both the more urgent medical problem and the greatest economic opportunity.
What Inflammatory Bowel Disease and Chronic Kidney Disease share in common is that they have “orphan drug” potential. When pioneering drugs for medical conditions for which there is no existing therapeutic options, the U.S. Food and Drug Administration (FDA) will designate drug research into such conditions as “orphan drugs” which is often a less expensive and faster process for gaining regulatory approval.
This provides an avenue for additional fast-tracking of the costly/expensive clinical trials process. Call candidates for these two conditions, “fast-tracking squared”.
NASH opportunity: “large drugmakers with piles of cash”
Investors wanting to know why the Company is so excited about its “NASH” research need look no further than a Reuters article from April 2017:
Large drugmakers with piles of cash are on the hunt for promising medicines being developed by small companies to treat NASH, a progressive fatty liver disease poised to become the leading cause of liver transplants by 2020.
“On the hunt” with “piles of cash”. Investors will like the sound of that. Titled [t]he next untapped pharma market…, Nash is in the process of tapping this market. And the Reuters article estimates this as a USD$20 to $35 billion market.
Junior technology companies seeking larger partners to help commercialize new discoveries usually find themselves standing at the back of a long line. According to Reuters, with Nash’s “NASH” research it will be Big Pharma that is queued outside the Company’s door awaiting results.
Inflammatory Bowel Disease (IBD)
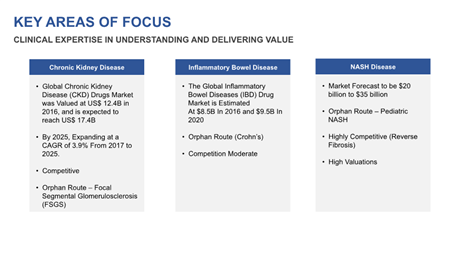
In aggregate, the global market to treat IBD was measured at USD$8.5 billion in 2016, estimated to reach USD$9.5 billion by 2020. For one particularly nasty form of IBD (Crohn’s Disease), orphan drug designation is also available – and this is the target of Nash.
Chronic Kidney Disease (CKD)
Last but not least in Nash’s lead R&D initiatives is its fast-tracking of a new treatment for CKD. The scenario here is similar to the IBD strategy. In aggregate, this is a USD$12.4 billion market globally, projected to grow to USD$17.4 billion by 2020. It’s also competitive, in terms of other pharmaceutical companies seeking to pioneer a new treatment.
Again, Nash’s strategy is to target a specific niche of the CKD disease (and CKD market): Focal Segmental Glomerulosclerosis (FSGS). The reason for this tactical approach is also similar: the opportunity for orphan drug designation.
Focusing on a smaller niche in these latter two markets means lesser overall revenue potential. However, the important trade-off is that if (when) orphan drug designation is obtained, the R&D is further expedited – improving the odds of getting to market first with a new treatment.
(click to enlarge)
In Parts 1 and 2, investors have been presented with the Nash Pharmaceutical business model in terms of what it is, how Nash plans on executing on this business plan, and where the Company currently sees its best opportunities to fast-track its pharmaceutical research.
In the concluding installment of this series, investors will have the opportunity to connect the dots. Stockhouse will take a look at some other success stories of smaller pharmaceutical companies that have “hit a home-run” with their own R&D. We’ll also examine the outlook for Nash and offer investors some clues on what to expect in the near future.
breathtecbiomedical.com
Nash Pharmaceuticals 3: Strong Bet for Multi-Bagger Payoff
 As Stockhouse presents its multi-part series on Nash Pharmaceuticals (a wholly-owned subsidiary of Breathtec Biomedical Inc. (CSE: BTH, OTCQB: BTHCF, Forum), investors have had a chance to absorb this unique business model piece by piece. In the concluding installment, we connect the dots: huge revenue potential, real-world examples of this drug repurposing strategy in practice, and several key investment drivers.
As Stockhouse presents its multi-part series on Nash Pharmaceuticals (a wholly-owned subsidiary of Breathtec Biomedical Inc. (CSE: BTH, OTCQB: BTHCF, Forum), investors have had a chance to absorb this unique business model piece by piece. In the concluding installment, we connect the dots: huge revenue potential, real-world examples of this drug repurposing strategy in practice, and several key investment drivers.
In Part 1, readers got the Big Picture. Via the Company’s “drug repurposing” strategy, Nash can bring old drugs to a patent-ready stage and into human clinical trials with maximum efficiency in terms of both time and cost.
This is due to the fact that the repurposed drugs at the heart of this new R&D have already been approved. This means much of the discovery and pre-clinical work has already been done. This can save up to 8 years in development time and potentially reduce costs by $10’s of millions.
(click to enlarge)
In Part 2, investors got important details on how Nash can execute on this strategy. Via Chief Scientific Officer, Dr. Mark Williams, the Company has identified 13 drugs that are potential repurposing candidates. With 7 of these, the data is already in place to commence fast-tracking into Phase II clinical studies.
Even more specifically, Nash has three R&D initiatives that it has targeted for immediate fast-tracking:
- Non-Alcoholic Steatohepatitis (NASH disease)
- Inflammatory Bowel Disease (IBD)
- Chronic Kidney Disease (CKD)
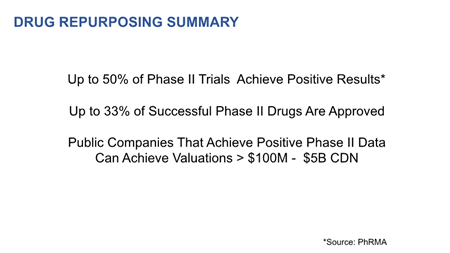
The significance of advancing to this stage has been explained, but for readers who missed the previous installments there are two important investment drivers here. Up to 50% of Phase II trials achieve positive results, with up to 33% of successful Phase II trials resulting in approved drugs [Source: PhRMA]. For this reason, such drug research already has significant commercial potential once R&D reaches this stage.
More efficient research for Nash = a faster payoff for shareholders. But this still misses the beauty of this business model.
Maximizing success/minimizing risk
The Nash approach to pharmaceutical R&D is not merely a much faster/less expensive model to fast-track drug development. It also allows the Company to enter this R&D process when the odds of success are maximized.
(click to enlarge)
Roughly 90% of new drug research initiatives never even reach a Phase I study – where research shifts to actual testing on human patients. Not only does the Nash repurposing model chop out much of the time and expense for drug development, it also ratchets down the level of risk for both the Company and its shareholders.
Costs (and time) are minimized. The odds of success are maximized.
It’s a formula for pharmaceutical success. In Part 3, we see how drug repurposing (and drug “repositioning”) can become a payoff in the $100’s of millions for a junior pharma company. For the larger pharma companies that commercialize these drugs, the revenue streams can be in the billions of dollars.

(click to enlarge)
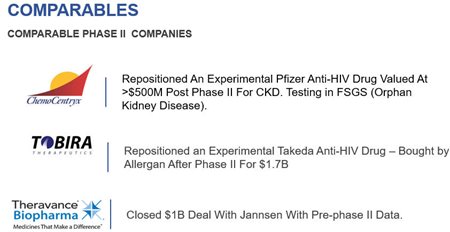
Biogen repurposed an (old) psoriasis drug into a (new) multi-billion treatment for multiple sclerosis.
Medivation repurposed an anti-histamine as a new treatment for Alzheimer’s disease and sold it for $400 million before completing a Phase III trial.
Celgene repositioned Thalidomide from being a (failed) morning sickness drug to a multi-billion dollar treatment for both leprosy and cancer.
Victoria-based Aspreva Pharmaceuticals repurposed a Roche Pharma drug for an “orphan indication” and then sold it for $915 million in 2007. At the time, it was a record for a made-in-Canada pharmaceutical product.
There are several take-aways here for investors. Generally speaking, we see how drugs previously developed for relatively mundane medical problems can be transformed into treatments for some of the most dangerous or debilitating medical conditions – with commensurate payoffs. However, the latter example is perhaps most instructive.
Like Aspreva, Nash also has great interest in orphan disease designations. Where no suitable therapy exists for a medical condition, the U.S. Food and Drug Administration (FDA) can designate a development-stage drug as “an orphan drug”, providing additional streamlining for R&D that can reduce time/costs even further.
Both Nash’s IBD research and CKD research have potential “orphan indications”. This means more than just greater efficiency. As perhaps the new standard of care for these diseases, there is fast-track commercialization potential in what are multi-billion dollar treatment markets.
(click to enlarge)
As exciting as those two initiatives are, most investors will be even more interested in Nash Pharmaceutical’s research into a new treatment for NASH disease. As noted in Part 2, the payoff for success here has already been telegraphed in a Reuters article from April 2017.
Large drugmakers with piles of cash are on the hunt for promising medicines being developed by small companies to treat NASH, a progressive fatty liver disease poised to become the leading cause of liver transplants by 2020. [emphasis mine]
That’s two lead research initiatives with orphan drug potential for the Company. However, those still take a back seat behind its NASH disease research, where the healthcare sector (and pharmaceutical industry) are clamoring for a new treatment to bring to market.
That clamor has never been louder. The Patent Cliff is the name the pharmaceutical industry has attached to a revenue-hole for Big Pharma that now totals in the $100’s of billions – due to the expiry of patents on a long list of major revenue producers.
With drug development far more expensive and time-consuming than ever before, Big Pharma has never been so eager to partner with junior pharma companies to replenish its pipeline. Here, astute investors will have already figured out an additional synergy in this business model.
Natural partners for commercialization
As noted, the pharmaceutical industry has a near-insatiable appetite today for new drugs that can be patented and commercialized. In the case of repurposing, however, particular drug companies will be especially interested in these new commercialization opportunities: the original drug developers.
With full infrastructure in place to manufacture these repurposed drugs along with existing distribution channels, acquiring repurposed drugs can be extremely lucrative for these companies. This translates into larger (potential) paydays for Nash and its shareholders. Not only might the original developers be willing to pay more for these repurposed drugs, they will also probably bid for them sooner.
If you’re the CEO of a drug-maker, watching a junior pharma company (like Nash) working to repurpose one of your drugs – with a new patent in play – the last thing you would want to see is one of your Big Pharma competitors jump in and grab that patent. Acquiring such drugs earlier and completing the R&D in-house (if necessary), could forestall a much more costly bidding war down the line.
(click to enlarge)
With Nash ready to commence fast-tracking on its lead initiatives, the Company plans on moving quickly. More news was just released on December 3, 2018: very strong results in pre-clinical work on its lead IBD initiative for Crohn’s disease. Not only did its lead compound (NP-178) exceed the current standard of care in some measures, Nash researchers have discovered a second compound (named “NP-120”) that delivered comparable results.
Drug repurposing. The Patent Cliff. Orphan drugs. Nash Pharmaceuticals. For tech investors looking to cash in on pharma opportunities, those first three terms will be invaluable in your due diligence. And after such education, the Nash business model will look even better.
breathtecbiomedical.com
FULL DISCLOSURE: Breathtec Biomedical Inc. is a paid client of Stockhouse Publishing.